For AR People exists to connect people to the policies that affect them. We want Arkansans to know when policies can make their lives better, and just as importantly, when their lives will be negatively affected by the people in power. Put simply, Arkansans deserve to know about what the government is doing with our time, tax dollars, and lives.
It was with this value of populism for the people of Arkansas that we decided to support the Arkansas Abortion Amendment.
The current abysmal state of women’s healthcare in Arkansas is a large part of why this amendment is necessary, no matter where you stand on the issue of abortion. So let’s look at the facts.
Arkansas is the most dangerous place to be a pregnant woman and the third most dangerous place to be a newborn baby.
Maternal mortality in Arkansas is higher than anywhere else in the country. This means women in Arkansas are more likely to die in pregnancy than in any other state.
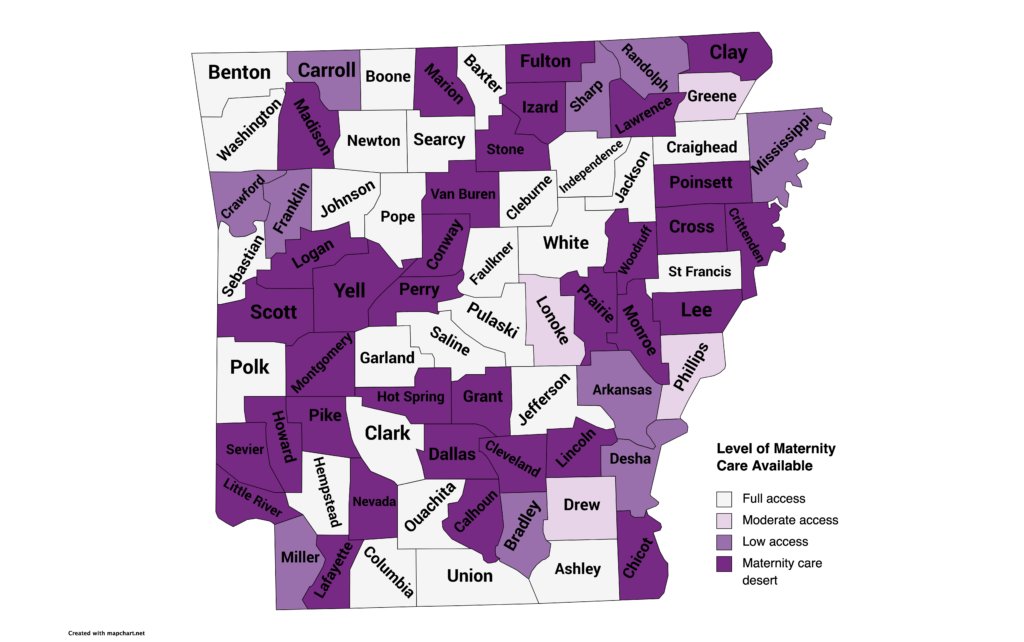
To get a complete picture, we can also view maternal danger through a lens of access to maternity healthcare. Nearly half the counties in Arkansas meet the definition of “maternity care deserts.” Such places are defined as “counties without any hospitals or birth centers offering obstetric care and without any obstetric providers.”
Arkansas also has serious problems providing prenatal care early enough. Early prenatal care is a primary determinant of positive pregnancy outcomes — the earlier in the pregnancy that a woman obtains prenatal care, the higher her chance of good outcomes.
The March of Dimes 2023 maternal care report shows over 1/5 of pregnant Arkansans (20.1%) either (1) did not receive prenatal care until the fifth month of pregnancy or later or (2) received less than 50% of the appropriate number of prenatal visits. The inadequacy report shows this is almost five points higher than the national average of 15.5%.
Arkansas has the third highest infant mortality rate in the country, which the CDC defines as the number of deaths prior to a baby’s first birthday divided by total number of births. This means that Arkansas is not only the most dangerous place to be pregnant or a new parent, we are also one of the most dangerous places to spend one’s first year of life.
Arkansas’s maternal and prenatal healthcare system is not even taking care of the babies that are born in the state. So much for being the most “pro-life” state.
What does Arkansas’s bleak maternal care reality have to do with abortion?
Hyper-partisan organizations and individuals tend to extract the issue of abortion from Arkansas’s dangerous maternal health care reality. The truth is, lack of access to abortion is correlated with high maternal mortality.
States where abortion was restricted in 2020 saw an average of 28.8 maternal deaths per 100,000 births. Compare this with the average of 17.8 maternal deaths per 100,000 births that occurred in states with abortion access. This gap has widened since trigger laws went into place in several abortion-restricted states in the wake of the overturn of Roe v. Wade.
Several factors contribute to the high maternal mortality rates in states with low or no abortion access. Many factors are related to other policies in the same states affecting outcomes of poverty, health, child care access, housing, food insecurity, and more.
Perhaps the most obvious factor that explains this correlation is the migration of doctors away from states like Arkansas, where abortion is illegal in virtually all circumstances.
Arkansans don’t have to be convinced that abortion is healthcare, but we would be foolish to ignore that that is the consensus among providers of maternal care. Providers of maternal care have their hands tied in states like Arkansas, where the evidence-based standard clinical practice has been criminalized by extremists with political power. In Arkansas, providers are not just at risk of losing their license—they can be fined $100,000 and sent to prison for 10 years.
According to the American College of Obstetricians and Gynecologists, pregnancy complications like placental abruption, bleeding from placenta previa, preeclampsia or eclampsia, and cardiac renal conditions can all require abortions in order to save a woman’s life or preserve her health.
To put this in experiential terms: A pregnant woman in Arkansas who experiences bleeding from placenta previa is given no options other than for her condition to continue to worsen until such a time as her doctor can, in consultation with the hospital legal counsel, administer the lifesaving care of abortion. The longer she goes without it, the higher the risk of sepsis or death, but the choice for when and if to administer an abortion is no longer up to the pregnant woman and her doctor. Arkansas doctors have been forced by extremist politicians to require an undetermined amount of suffering by their patient before administering an evidence-based standard of care: an abortion.
It is no wonder doctors flee states like ours.
It is no wonder maternal care is so scarce in states like ours.
It is no wonder half the state’s counties are maternal care deserts.
Arkansas, we have work to do. We have a goal to restore balance to the legislature so that reasonable policy can prevail in Arkansas lawmaking. That work, not matter what, will take several political cycles to achieve.
A Constitutional amendment is the only way to save the lives of women and girls who are currently in danger within the borders of Arkansas. The good news is, and always will be, we are a state with people power. The same Constitution we are trying to amend gives us a pathway to change it by the power of the people. Direct democracy will save us.


